

© Svitlana Belinska / Adobe Stock
By Jack Matter
| If you think you or someone you know is struggling with opioid misuse or addiction, free and confidential help is available. Call SAMHSA’s National Helpline at 1-800-662-4357. If you are experiencing a crisis, call 911 or the National Suicide Prevention Lifeline at 988. |
In late spring and early summer, vibrant flowers bloom by the hundreds in fields as far as the eye can see. Delicate petals sway gently in the breeze in pink, white, and signature bright red hues. These flowers have captivated the minds of gardeners and drug lords alike with their allure but for wildly different reasons. Yes, you did read that correctly, drug lords. Opium poppies, known to the botanists among us as Papaver somniferum, are both admired for their aesthetic appeal and valued for their role in the large-scale manufacture of narcotics. The gooey white extract from the seed pod of a poppy contains opiates, a potent group of chemicals exploited for their pain-relieving effects. This exploitation has given rise to the widespread—and often illegal—cultivation of opium poppies to make a potent drug class called opioids, which include morphine and heroin. So, how did we go from flower bud to pain relief?
Opiates have long been a cornerstone of pain management. The liquid extract from the opium poppy has a rich history of use as a natural painkiller spanning millennia, from the ancient Fertile Crescent to the modern day. By the early 1800s, Friedrich Sertürner, a pioneer in alkaloid chemistry, had isolated the specific compound morphine from the liquid. Even so, the precise way in which opioids work in our bodies is still not 100% known. We do know that opioids fundamentally alter the experience of pain by chemically binding to opioid receptors in the cells of our nervous system. It can be helpful to think of these receptors as a lock that only a specific opioid-shaped key can open. In order to be this key, opioids imitate the natural compounds in our body called endorphins, which you may be familiar with as the “feel-good” chemicals released by our brains when we do an activity like exercise. By mimicking the actions of feel-good chemicals, opioids can trigger major reward pathways in your brain over and over again, producing their painkilling and sometimes euphoric effects. As a result, opioids are potent tools that are frequently used in pain management.
Despite how ubiquitous they’ve become, the use of opioids for pain management is always a gamble, and the choice to both prescribe and use them should never be taken lightly. As a drug class, they carry a high risk of dependence, addiction, and ultimately overdose. When someone experiences these consequences, they suffer from an opioid use disorder. This means that they continue to misuse opioids long after they develop damaging physical, psychological, and interpersonal effects. The insatiable craving for opioids leads to a vicious cycle of abuse and withdrawal that is difficult to treat. The long-term consequences of opioid misuse extend far beyond individual health and have evolved into the widespread societal challenge we now call the opioid crisis.
The scope of the epidemic is truly staggering. Most cases of opioid misuse start with drugs that a healthcare provider prescribes, but many are also obtained illegally. Now, three million people in the United States meet the criteria for opioid use disorder. Without sugarcoating it, this is the result of over twenty-five years of overprescription, an ill-equipped healthcare system, and a lack of meaningful drug policy changes. The economic burden of the strained healthcare system and the social stigma associated with addiction contribute to the complexity of addressing these root causes. Vulnerable populations, including those with a history of substance abuse, individuals with mental health disorders, and socioeconomically disadvantaged communities, are particularly at risk of developing addiction, which only deepens the rift in healthcare disparities. Still, all hope is not lost.
Despite a reduction in the number of opioid prescriptions since the onset of the crisis, the overall number of opioid-related deaths has not declined. So, we need to look deeper into the opioid crisis from all angles. Experts agree that we must combine robust regulatory measures, improved access to evidence-based treatments, and widespread education on pain management to fight back. The stance that prescription is the issue’s root has some merit, but it’s time to look beyond prevention at just the script pad. Rather, this crisis should be treated as a symptom of a broader issue in a healthcare system that prioritizes a quick fix for very complex needs.

I won’t sit here and pretend to know exactly what to do about that. A lot of smart people who have dedicated their lives to solving this crisis are still searching for answers. Even if we just focus on the individual person, socioeconomic disadvantage and its relationship to chronic pain requires meaningful, long-term attention from healthcare providers. This is a formidable barrier in a system that both incentivizes profit and prioritizes high patient turnover rates. To achieve truly meaningful change, we likely need education on the structural causes of opioid abuse to become part of a national curriculum for healthcare providers.
In addition, access to evidence-based treatments, such as methadone, needs to be drastically improved. Methadone can reduce the harmful effects of opioid withdrawal and block the euphoric feelings that drug users chase. Despite this, in many states where the crisis is at its worst, access to methadone is severely limited by Medicare policy outlawing coverage for these treatments. Even when methadone and similar treatments are used, they rarely see widespread implementation. Scaling up these treatments in combination with preventative efforts could be a way to ease the opioid crisis from a routine clinical setting where the patient is at the center of their own care.
Of course, clinician education and access to treatments are only a couple of many things that need to happen to begin seeing a future free of this crisis. I don’t know about you, but I find all this very overwhelming. The slope certainly feels insurmountable from way down here. But that doesn’t mean we have to be complacent. Believe it or not, we all can create meaningful change in our communities.
How? Start with learning how to recognize the signs of opioid addiction and overdose. Opioid addiction drastically increases someone’s risk of overdose. Someone experiencing an opioid addiction can have some or all of the following signs and symptoms:
- Difficulty or inability to stop using opioids
- Taking more opioids or taking opioids for prolonged periods
- Spending less time in social situations due to drug use
- Experiencing cravings for opioids or withdrawal when not using
- Continuing to take opioids despite adverse health and/or social consequences
Opioid overdose is a life-threatening medical emergency, but it is treatable with quick actions. You should call 911 if you suspect someone is experiencing an overdose. Someone experiencing an opioid overdose may have some or all of the following signs and symptoms:
- Blue or purple lips and/or fingernails
- Pale, damp, and/or cool skin
- Unresponsive, even to shouting and/or pain
- Breathing that is slow, shallow, or stops completely
- Heartbeat that is slow or stops completely
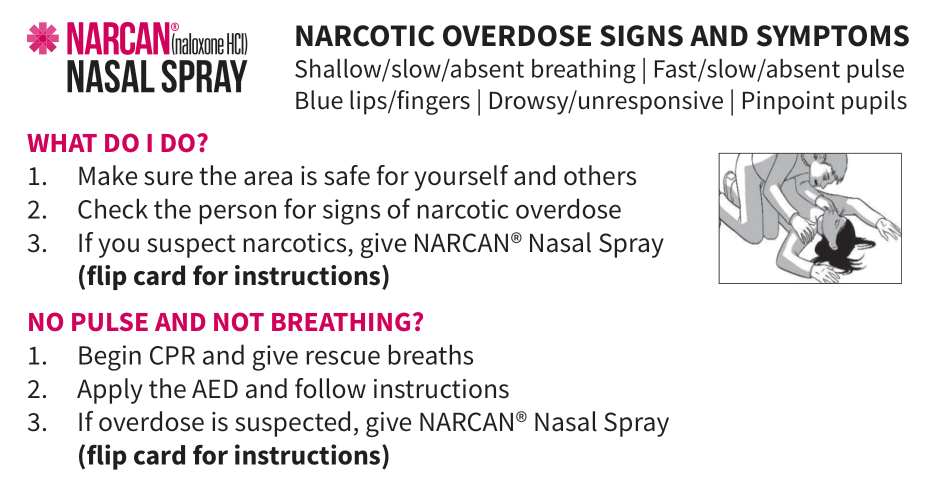
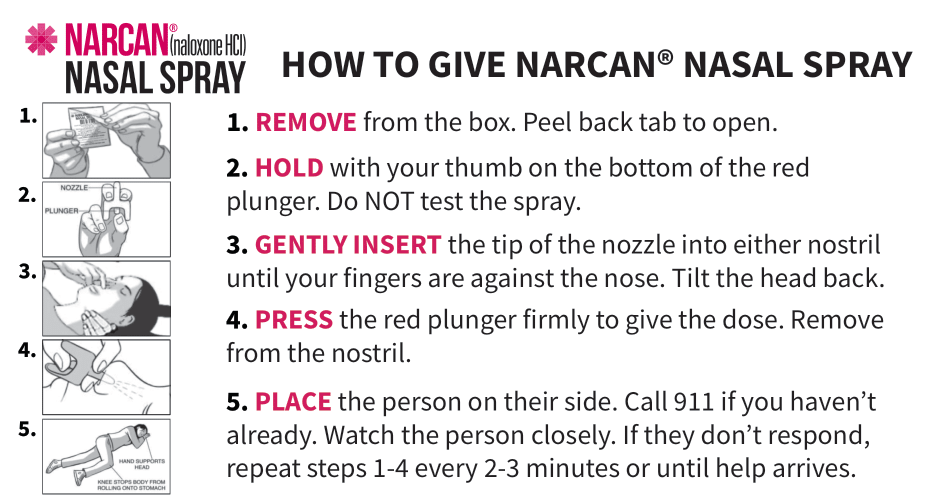
The CDC offers even more guidance on the signs of overdose, as well as indications that you or someone you know might be in a difficult spot with opioid misuse. Get trained and carry naloxone—the generic name of the NARCAN® nasal spray—which is a drug that can reverse an in-progress opioid overdose. You can probably get it for free in most places, even delivered to your doorstep, no questions asked. (P.S. as a bonus, I’ve even given you a convenient, printable NARCAN® pocket card below to go with it.) Learn your local and national resources, which you can start by looking at the principles of harm reduction. Who knows, you might just save a life.
Printable NARCAN® (naloxone) pocket card – just right click and save!
References
Blanco, C., Wiley, T. R., Lloyd, J. J., Lopez, M. F., & Volkow, N. D. (2020). America’s opioid crisis: The need for an integrated public health approach. Translational Psychiatry, 10(1). https://doi.org/10.1038/s41398-020-0847-1
Brunning, A. (2018, September 5). A brief guide to common painkillers. Compound Interest. https://www.compoundchem.com/2014/09/25/painkillers/
Brunning, A. (2023, November 15). The chemistry of poppies: Colours and opium. Compound Interest. https://www.compoundchem.com/2020/11/11/poppies/
Centers for Disease Control and Prevention. (2021, October 6). Preventing opioid overdose. Centers for Disease Control and Prevention. https://www.cdc.gov/opioids/overdoseprevention/index.html
Centers for Disease Control and Prevention. (2023, August 8). Understanding the opioid overdose epidemic. Centers for Disease Control and Prevention. https://www.cdc.gov/opioids/basics/epidemic.html
Chaudhry, S. R. (2023, April 3). Biochemistry, endorphin. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK470306/
Dasgupta, N., Beletsky, L., & Ciccarone, D. (2018). Opioid crisis: No easy fix to its social and economic determinants. American Journal of Public Health, 108(2), 182–186. https://doi.org/10.2105/ajph.2017.304187
Dydyk, A. M. (2024). Opioid use disorder. StatPearls [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK553166/
Mayo Foundation for Medical Education and Research. (2023, November 29). Am I at risk of opioid addiction?. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/prescription-drug-abuse/in-depth/how-opioid-addiction-occurs/art-20360372
National Harm Reduction Coalition. (2023, December 2). Harm reduction principles. National Harm Reduction Coalition. https://harmreduction.org/about-us/principles-of-harm-reduction/
Opium poppy. DEA Museum. (n.d.). https://museum.dea.gov/exhibits/online-exhibits/cannabis-coca-and-poppy-natures-addictive-plants/opium-poppy
Presley, C. C., & Lindsley, C. W. (2018). Dark classics in chemical neuroscience: Opium, a historical perspective. ACS Chemical Neuroscience, 9(10), 2503–2518. https://doi.org/10.1021/acschemneuro.8b00459
U.S. Department of Health and Human Services. (2018, June 5). How opioid drugs activate receptors. National Institutes of Health. https://www.nih.gov/news-events/nih-research-matters/how-opioid-drugs-activate-receptors
USDA plants database. (n.d.). https://plants.sc.egov.usda.gov/home/plantProfile?symbol=PASO2


